There's a bunch of underinsured (or outright not insured) folk in the very locations where Walmart is opening these, so it has the potential to kill a couple of different birds with one stone. From a public benefits side, it gives a path of medical care for those that otherwise wouldn't have it (beyond say, an emergency room visit). It also lower prices by competing against insurance bloat.
In doing so, Walmart (may) be able to create a sustainable business by tapping a market (folk that aren't currently going for medical coverage anyway) that would otherwise be untapped.
This could also control costs if government managed systems (Medicare, Medicaid) partner with Walmart to provide payment. Easier to negotiate with Walmart as a single entity versus a network of vision and dental providers across the nation.
In Canada the govt doesn’t provide healthcare. It sets public rates for services, and then providers can provide those services to the public and get paid the set rates by the govt. This is called “single payer healthcare”.
You're right - for specialists and some GPs but not all. About half of the GPs are paid by their roster size, so-called "capitated payment". The idea being a doctors pay should be based on how healthy they keeps their patients rather than how many services they administer.
I only point that out for our American friends who might counter with "well isn't that a system ripe for abuse"
Really, do you have a source for that? I assumed everything, basically everything public insurance driven, which are most things, are negotiated by the government.
Just like how family/walk-in doctors get paid in 15 minutes increments so they try to rush as many patient through the day since they get paid for 15 whether it was a 2min appt or not. Which is why you see walk-ins packed full of people with well over an hour times, because not every meeting is fast.
On the other hand, I assumed the specialist got paid for their individual services they provide (and the orignal doctor got rewarded for the referral), since that's what they get referred to do, a specialized service which can be rated. It's also why radiologists ($800k/yt) are the highest paid doctor-type, complicated stuff requires good pay and they negotiate these on a case-by-case basis.
Edit: I found a paper talking about capitation in Canada and it mentions that Ontario is the only pr]ovince doing it and not all GDPs opted-into it. This sounds interesting - if a bit trusting of the people reviewing "performance". But I support testing out new payment systems, the current one could use some optimisation no doubt.
Same in Switzerland. Prices for services are fixed, and mandatory basic insurance won't pay more. Doctors and private hospitals are free to do their own thing, as long as their clients (or their additional insurance) are willing to pay the difference. I think only hospitals are in public hand, but they still have to go via the insurances for payment.
That’s certainly an option, but the meta-question is: which mechanism can produce health/pharma goods and services at lower costs and higher quality, markets or government allocation?
If the answer is the latter, then why aren’t we replicating that mechanism across other essential goods like food and clothing?
Some relevant questions are whether the demand is elastic and how difficult to compare and/or fungible the product is. Medical care is inelastic (without it you die) and difficult to compare (you don't get to try the same surgery with two different providers). Food is inelastic (even more so), and easy to compare, but many foods are very fungible (your supermarket will let you choose red white or yellow onions, but not which farm your onions come from). Demand for clothing is more elastic (you need it but you can probably wait for a sale), and it's easy to compare the items.
Medical care can be difficult to compare, but is that necessarily true across ALL medical care? There exists a high degree of fungibility in most preventive care: routine treatments like annual physicals, bloodwork, antibiotic prescription, flu shots, diagnostic imaging, etc.
The next question is: is there the same degree of fungibility for more major care, like tonsillectomies and appendectomies? Perhaps brain surgery and oncology is less fungible — but they are also perfect candidates for insurance coverage since they're catastrophic.
Same is true for food. I also wonder how affinity analysis can be applied to medical care. And - can the question of market vs government allocation be analyzed using "baskets"?
Most healthcare is not for life threatening illness. The bigger problem in healthcare in the US is that consumers almost never know how much a service will cost beforehand.
A "pure" competitive market would, but we don't have that and we're not going to get it. Eliminate insurance "networks", force hospitals to publish price lists and give the same price to every patient, make the medical statistics of every hospital and provider publicly accessible, and costs will plummet. As of now we have a hybrid system that combines the worst of both methods.
I think that's the key point. That would give insurances much more leverage to negotiate lower prices for everyone. Even other smaller insurances would profit... which would increase competition between the insurances... which would lower insurance costs for the people.
>then why aren’t we replicating that mechanism across other essential goods like food and clothing?
maybe because the competition doesn't work as well in healthcare sector? or that there isn't a whole scheme of inflated prices that insurance companies negotiate down to, but uninsured people are forced to pay?
If that's the case, then why are we seeing Wal-Mart attempting to compete in the healthcare sector with what seem to be competitive prices?
Doesn't seem to be limited to just Wal-Mart either. An Oklahoma City Hospital began posting its prices online and started a bidding war[1]. The hospital lobby seems to be overwhelmingly opposed to price transparency out of fear that it will lower prices[2], and there are Yelp-like directories that are beginning to provide price transparency allowing for competitive rates like $79 MRI's[3].
Walmart actually made a big difference in the health market years ago when they introduced the $4 prescription program, something like 300 pharmaceuticals that are available for $4. Even for people with health insurance this is lower than many insurance providers' co-pay pricing.
>If that's the case, then why are we seeing Wal-Mart attempting to compete in the healthcare sector with what seem to be competitive prices?
And it only took decades of skyrocketing healthcare costs (and probably margins) for walmart to enter the space. How many more decades (if ever) until prices drop down to level in line with other developed nations?
> And it only took decades of skyrocketing healthcare costs (and probably margins) for walmart to enter the space. How many more decades (if ever) until prices drop down to level in line with other developed nations?
Was this a natural consequence of the market, or are there other explanations for why such a delay came to pass?
Why is this question relevant? Let's say the reason was that walmart thinks their core competency is supply chain management, healthcare isn't part of that, and they only entered because the healthcare industry gravy train has reached insanely high levels that they simply could not refuse, what then? Should our response to this crisis be to wait until a megacorp comes by and saves the day?
This question is extremely relevant, because it can help us evaluate all policy options.
The current status quo in the US Healthcare system was not some crazy accident of the market, rather it was the inevitable result of a series of policies passed at state, local, and federal levels over the past half century.
The fact that health insurance isn’t portable, and is rather tied to employment is a consequence of the WW2 era wage ceilings imposed on private corporations, followed by the tax benefits enjoyed by employers that provide group insurance, followed then by the mandate on employers to provide health insurance. This is in contrast with other countries that employ private insurance, like the Netherlands and Switzerland, where insurance is tied to the individual, not the employer.
The lack of price transparency logically follows from the fact that patients never really care how much their treatments cost, since employer sponsored insurance covers everything anyway. Large corporations are less price sensitive than individuals, which exacerbates the price inflation over decades.
Certificate of need laws, where local hospitals get to decide if a new, competing hospital can open, and the residency system requiring 10+ years of schooling to practice resulted in inevitable supply constraints.
Medicare, which provides healthcare for free for the elderly, removed the most engaged buyers from the market, suffocating the price discovery mechanism. Not only that, the elderly tend to be the richest people in the country - those above the age of 55 account for 73% of wealth in America. Boomers are disproportionately rich, and yet they also enjoy some of the most generous welfare on top of that.
There are number of ways to approach solving this problem. One way is to add yet another band-aid on top of the system, burn down the system entirely, or identify the root causes and disentangle them from the system. This is the political question.
>The fact that health insurance isn’t portable [...]
Agreed.
>This is in contrast with other countries that employ private insurance, like the Netherlands and Switzerland, where insurance is tied to the individual, not the employer.
It's worth mentioning that in both countries, there's heavy government regulation. According to wikipeida, in the Netherlands 50% of premiums goes to some sort of government agency that redistributes money to private insurance companies depending on their claims, which makes it a quasi-public payer scheme. In Switzerland the premium is capped at a percentage of a person's income with the government making up the shortfall, and insurance companies can't make a profit.
>The lack of price transparency logically follows from the fact that patients never really care how much their treatments cost, since employer sponsored insurance covers everything anyway.
Doesn't this argument apply to insurance schemes in general, both public and private?
>Large corporations are less price sensitive than individuals, which exacerbates the price inflation over decades.
I'm skeptical about this claim. Sure, they have more money sloshing about than individuals, but insurance premiums across the entire workforce adds up.
>Certificate of need laws, where local hospitals get to decide if a new, competing hospital can open, and the residency system requiring 10+ years of schooling to practice resulted in inevitable supply constraints.
Agree, although I'm weary of assigning significant blame due to this factor. Are doctors making record wages? Are hospitals making record profits?
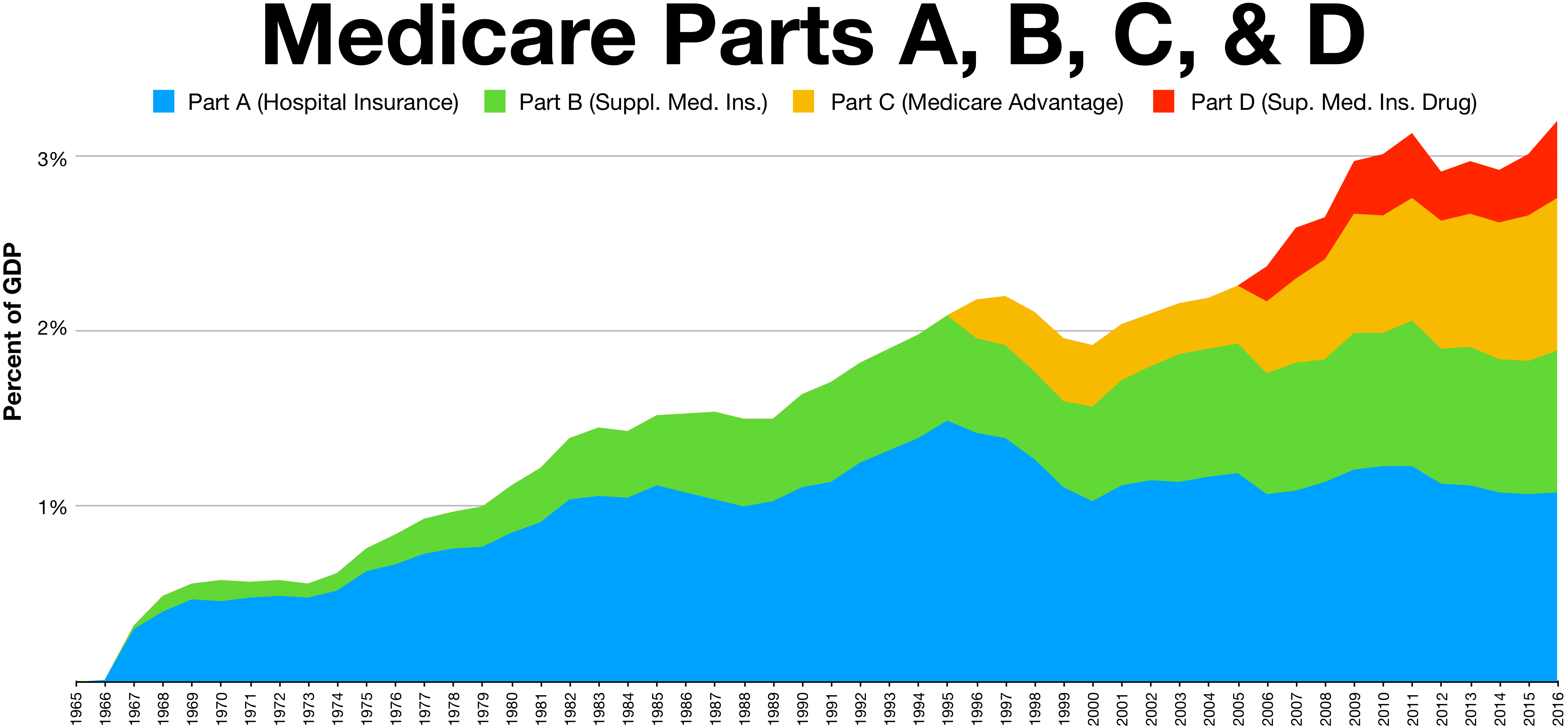
>Medicare, which provides healthcare for free for the elderly, removed the most engaged buyers from the market. Not only that, the elderly tend to be the richest people in the country - those above the age of 55 account for 73% of wealth in America. Boomers are rich, and they also enjoy some of the most generous welfare on top of that.
I'm skeptical how big of an effect this can be. Wikipedia has a chart that shows medicare spending as percent of GDP[1]. If you combine that with total US healthcare spending by GDP[2], you see that it accounts for less than a fifth of total US healthcare spending.
> It's worth mentioning that in both countries, there's heavy government regulation
No disagreements that there exists regulation that can be helpful. Definitely an important part of the discussion. Even in Singapore, which is largely a market based system driven by price discovery relies on a healthy (heh) amount of regulation. In the US, the food system is largely market-based, but the FDA (as well as state and local health departments) impose important regulations.
> In Switzerland the premium is capped at a percentage of a person's income with the government making up the shortfall, and insurance companies can't make a profit.
Keep in mind that in the US, health insurance companies report an average profit of ~5%. Even if you eliminated that entirely, you wouldn't see any savings worth writing home about. I work at an insurance company, and the majority of claims I see are pretty asinine. $500 added to provide sign language service to a deaf patient, or $300 charged for a papoose used while giving a child a cleaning. Because of the third-party-payer model in which the care is priced and paid for AFTER the services are rendered, the patient has little skin in the game. In the best case (for the patient) the insurance company simply pays the asking price (resulting in a sort of moral hazard), and in the worst case, the insurance company doesn't cover it and the patient gets a surprise bill in the mail.
> Doesn't this argument apply to insurance schemes in general, both public and private?
Yes, it's another reason why using insurance to pay for all care can be a sub-optimal way to allocate resources. Not having skin in the game can result in patient overconsumption.
> Agree, although I'm weary of assigning significant blame due to this factor. Are doctors making record wages? Are hospitals making record profits?
Yes, and yes[1][2]
> I'm skeptical how big of an effect this can be. Wikipedia has a chart that shows medicare spending as percent of GDP[1]. If you combine that with total US healthcare spending by GDP[2], you see that it accounts for less than a fifth of total US healthcare spending.
The effect I'm talking about is removing the largest consumers of healthcare (rich old people) from the market, which impacts how the ultimate price of goods/services is determined by the market.
Clothing is a wildly different market. Imagine if the only way to get clothes were through a bespoke tailor, in person. No other way. And you often had—had—to get a very specific kind of jacket or whatever, no option to sub some other article, or else you or your kid dies or lives in pain or something. That’s healthcare. If clothes worked that way that market would suck, too.
Explain France and Switzerland then. Both use market mechanisms for delivering outpatient care. Or are these not European nations with universal healthcare?
Limiting the question to price and quality but ignoring availability might (I don’t know) favor markets and definitely ignores an (arguably) basic obligation of government but not markets.
I’d argue that the basic obligation of the government is welfare, at its core. Everything else is an implementation detail in service of that.
If the (regulated) market can bring down equilibrium prices to the minimum, then the government’s role could be to provide health stamps or cash to those in need, similar to food stamps (which can arguably be reformed).
I think that’s a fair expectation of government. It may be that the market can deliver care at the lowest cost but what if the market delivers that lower cost by limiting supply? Say they don’t offer service in some areas or limit some procedures?
Then the next question is: historically, which systems of resource allocation have been able to successfully avoid supply shortages of the thing in question, markets or government allocation?
Market prices are currently set based on 1-3x multipliers of Medicare reimbursement, so by definition the government already handles health care at lower costs.
Commodifying health care has proven to be disastrous in the US because it's, in practice, impossible to "shop around" — not even including cases where the "customer" is unconscious or in a life-threatening situation where "shopping" would be ridiculous, the profit models of health care centers are forcing many to close, leaving people with few choices in their immediate area, exacerbated by the "network" coverage model of insurance companies where you may not even be able to go to certain hospitals or doctor's offices.
Interestingly, though, improvements in supply chain management are making it possible to centrally-plan commodities like clothing. Multinational companies like Wal-Mart and Amazon are doing this already, in fact.
> Market prices are currently set based on 1-3x multipliers of Medicare reimbursement, so by definition the government already handles health care at lower costs.
I work in insurance, and I can tell you right now that $25 for a cleaning (per this article) is significantly lower than the amount for a cleaning (procedure code D1110) set by Medicare/Medicaid. You can look it up yourself by visiting the FAIR Health code lookup tool (https://www.fairhealthconsumer.org/dental/results), and setting the ZIP code to that of Carlton, GA (location of the Wal-Mart clinic), 30627. The average allowed amount is $64.
> Commodifying health care has proven to be disastrous in the US because it's, in practice, impossible to "shop around" — not even including cases where the "customer" is unconscious or in a life-threatening situation where "shopping" would be ridiculous, the profit models of health care centers are forcing many to close, leaving people with few choices in their immediate area, exacerbated by the "network" coverage model of insurance companies where you may not even be able to go to certain hospitals or doctor's offices.
Ignoring emergency health services (which is the minority of health spending), I'm not sure that we have enough information to irrefutably prove that preventable and planned care cannot be successfully commodified. A common theory around why we haven't been able to commodify healthcare in the US is due to a lack of price transparency, and the fact that employer sponsored health insurance removes the price sensitivity from buyers[1][2].
> Interestingly, though, improvements in supply chain management are making it possible to centrally-plan commodities like clothing. Multinational companies like Wal-Mart and Amazon are doing this already, in fact.
They aren't centrally planned, though — they are subject to market competition (see: DHL, UPS, FedEx, FlexPort, Maersk, etc). Their ability to be major "central planners" by controlling large parts of the supply chain is predicated on their ability to fend off market competition, and the moment they fail to do that, this manifests as a market opportunity for new competitors to take their place, wherever in the supply chain the large corporations fall short.
> If the answer is the latter, then why aren’t we replicating that mechanism across other essential goods like food and clothing?
We do/have. Water, electricity, phone services (and other communication), roads, child care and and whatever else the romans have done for us have all had successful government implementations. Food and clothing typically haven't been included in this list because choice is more important for them and the market does a good job at providing them, but even there I think there's room for a government foodbank/clothes bank style option.
> Water, electricity, phone services (and other communication), roads
These are all natural monopolies due to the limitations of public infrastructure. Such natural monopolies don't necessarily exist for goods/services like food, clothing, and medicine (most notably, over-the-counter generic medicine). Communication is largely left to the market, rather than government coordination/pricing.
> but even there I think there's room for a government foodbank/clothes bank style option.
Either that, or just providing the poor with money to buy food at market-rates, i.e. food stamps.
Notably, food and to some extent clothing (textiles) have been very much the concern of the state, or of the way the state’s organized. What’s changed is that both got way the hell cheaper to make and we settled on some good, more-or-less stable regulations and systems of management to keep things from getting too nutty too fast.
Government doesn't provide service directly almost anywhere else in the developed world. Especially the services Walmart is targeting (optometry, dental cleaning, etc).
Universal coverage doesn't mean government employs every provider directly.
{kind=link}
There's a bunch of underinsured (or outright not insured) folk in the very locations where Walmart is opening these, so it has the potential to kill a couple of different birds with one stone. From a public benefits side, it gives a path of medical care for those that otherwise wouldn't have it (beyond say, an emergency room visit). It also lower prices by competing against insurance bloat.
In doing so, Walmart (may) be able to create a sustainable business by tapping a market (folk that aren't currently going for medical coverage anyway) that would otherwise be untapped.